Johns Hopkins Global mHealth Initiative, 2016 Annual Report (Page 32-33)
Author: Nishant Singh


Telemedicine for continued delivery of essential health services
Source: Livemint
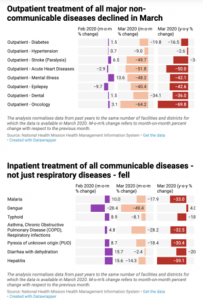
The COVID-19 pandemic has completely disrupted the delivery of regular health services in rural areas and put an enormous burden on the healthcare system. This stress on the public health system is going to result in increased maternal and child mortality, deaths due to non-communicable diseases, deaths due to malaria, reduced immunization rates, higher birth rates due to poor access to family planning, etc.
The COVID-19 pandemic has placed increased importance on the role of telemedicine in the delivery of routine healthcare services. Remote healthcare minimizes direct contact between a patient and a provider and reduces the risk of infection transmission. It also allows for the decongestion of healthcare facilities. The WHO includes telemedicine as an important component of “Maintaining essential health services: operational guidance for the COVID-19 context (June 2020)” and recommends shifting the delivery of rousing services to digital platforms
Hence, in the light of the current pandemic, guidelines have been issued for patients to seek medical consultations with healthcare providers on phone first and only then visit in-person if the healthcare provider deems that an in-person visit is necessary. As much as possible, the use of remote healthcare is encouraged for the delivery of essential health services.
We’re working with state governments, district governments, and NGOs in India to set up telemedicine projects in rural areas by strengthening the Ayushman Bharat program. This project aims to create a telehealth network that connects Health and Wellness Centers (HWCs) under Ayushman Bharat [i.e. Primary Health Centers (PHCs) & Sub centers (SCs)], or Spokes, with a nodal Medical college, or Hub, to deliver essential health services related to COVID and essential health services like ANC care, child health, first aid, etc.. Thus patients can get appropriate advice for home-based care and appropriate referrals for management via telemedicine at the HWC level itself. We have partnered with Aaroogya Foundation to create a network of on-demand remote doctors with 200+ active doctors from 20+ different specializations like General Medicine, Pediatrics, Cardiology, Obstetrics & Gynecology, Orthopedics, ENT and Neurology. Here’s a short video explaining how our technology and our model works.

Other Blogs
What are the medicolegal implications of India’s new telemedicine guidelines?
BY NIKHIL ISSAR, CONTRIBUTING AUTHOR, PSA
On March 25, 2020, the Ministry of Health and Family Welfare, Government of India issued the Telemedicine Practice Guidelines (“Guidelines”) appended as Appendix 5 to the Indian Medical Council (Professional Conduct, Etiquette and Ethics) Regulations, 2002 (“Ethics Regulations”). The promulgation of the guidelines has met the longstanding demand for the regulation of health consultation by virtual means between doctors and patients and places India amongst a select few jurisdictions that have a telemedicine regulation. These FAQs capture some key questions that have come up from patients, doctors and technology platforms.
What is telemedicine?
Telemedicine is defined as the delivery of health-care services, where distance is a critical factor, by all health-care professionals using information and communications technologies for the exchange of valid information for the diagnosis, treatment, and prevention of disease and injuries, research and evaluation and the continuing education of health-care workers, with the aim of advancing the health of individuals and communities. In other words, telemedicine means the delivery of health care services and clinical information by health-care professionals using telecommunication technologies such as the internet, wireless, mobiles and telephone media.
Is there any difference between telemedicine and telehealth?
Yes, telemedicine denotes the clinical service delivered by a medical practitioner whereas telehealth is a broader term that refers to the use of technology for health and health-related services including telemedicine.
Who can provide telemedicine facilities?
Only a Registered Medical Practitioner (“RMP”) i.e. a person who is enrolled in the State Medical Register or the Indian Medical Register under the Indian Medical Council Act, 1956 can practice telemedicine in India. Further the same professional, ethical norms and standards shall apply to any RMP providing telemedicine.
RMPs who seek to practice telemedicine must get themselves conversant with the provisions of the guidelines as well as with the process and limitations of the practice. For this purpose, a mandatory 3-year online course shall be conducted by the Board of Governors. However, in the interim period any RMP can practice telemedicine by adhering to the provisions of the Guidelines.
What are the modes of communication that can be used by RMPs?
RMPs can use various communication tools such as telephone, video, devices connected over LAN, WAN, Internet, mobile or landline phones, WhatsApp, Facebook Messenger, etc., or Mobile apps or internet-based digital platforms like Skype/ email/ fax, etc. for telemedicine. The use of different tools is dependent on the context; seriousness, urgency, and stage of consultation as each of these technologies have their respective strengths and weaknesses that may be appropriate or inadequate to deliver a proper diagnosis. Further, as specified below, RMPs cannot prescribe certain medicines if the mode of consultation is not through video-conferencing.
Who can avail telemedicine consultations? What are the services that can be provided by the RMPs?
RMPs can provide telemedicine consultation (hereinafter referred as “teleconsultation”) to patients from any part of India. The Guidelines do not cover consultations by RMPs outside of India, and the same may be regulated by applicable foreign law. RMPs can provide:
(i) Health education: imparting health promotion and disease prevention messages related to diet, physical activity, cessation of smoking, contagious infections, advice on immunizations, exercises, hygiene practices, mosquito control, etc.
(ii) Counselling:includingfoodrestrictions,do’sanddon’tsforapatientonanticancerdrugs, proper use of a hearing aid, advice for new tests, home physiotherapy, etc. to mitigate the underlying condition.
(iii) Prescribe Medicines as specified below.
What are the kinds of medicines that can be prescribed to a patient? Do the patients get a copy of the prescription?
RMPs can prescribe medicines only after they are satisfied that adequate and relevant information about the patient’s age (in case of doubt, RMPs can seek age proof), and medical conditions have been collected. In cases where a physical examination is necessary, RMP is barred from prescribing medicines until a physical examination can be arranged. Any prescription given without appropriate diagnosis would amount to professional misconduct.
RMP has to provide the patient with a copy of the signed prescription and can send the prescription directly to a pharmacy if the patient explicitly consents. This enables the patient to get the medicines from any pharmacy of his choice. However, there is a limit to the kind of medicines that can be prescribed via telemedicine. The medicines that can be prescribed are:
Over-the-counter medicines (List O) such as paracetamol and medicines required during a public health emergency.
(List A) Medicines such as for hypertension and skin problems that are prescribed during the first consultation via video consultation, and thereafter their re-fill can be prescribed through other communication modes.
(List B) Medicines as follow-ups for treating chronic diseases can be prescribed through follow-up consultation, after an initial in-person consultation has taken place.
However, medicines that have a high potential of being abused such as those listed in Schedule X of Drug and Cosmetic Act, 1940 and Rules or any Narcotic and Psychotropic substance listed in the Narcotic Drugs and Psychotropic Substances, Act, 1985 cannot be prescribed via telemedicine.
Will telemedicine replace physical examination?
No, consultations over audio, video or the internet cannot replace physical examination. RMPs have to exercise their professional judgment to decide whether a teleconsultation is appropriate or in-person consultation is needed. If a physical examination is critical, then the RMP should not proceed with teleconsultation until an in-person physical consultation has been arranged.
However, in case of emergencies where there is a lack of any other alternative, RMPs can provide teleconsultation to the best of their judgment. Thereafter, the patient must be immediately referred for in-person consultation.
Can RMPs force a patient for telemedicine? Are minors allowed to use telemedicine?
An RMP cannot insist on telemedicine if a patient is ready and willing to come to a physical facility. Patients have to provide their explicit or implicit consent for availing teleconsultation. Consent is said to be implied when the patient requests the consultation. On the other hand, patient’s explicit consent is required when a health worker, RMP or a caregiver initiates the consultation. Explicit consent can be given by the patient via email, text or audio/video message to the RMP (For e.g. “Yes, I consent to avail consultation via telemedicine” or any such communication in simple words). RMP is required to record the consent in his patient records.
In the case of minors, telemedicine is allowed only when the minor is consulting with an accompanying adult whose identity has been ascertained by the RMP.
Can anonymous teleconsultation be done?
Anonymous teleconsultation is not allowed by the guidelines. Identity disclosure and verification of both the patient and the RMP is necessary for availing/providing the services. RMP is required to collect and verify the patient’s personal information such as name, age, address, phone number, email Id, registered ID or any other identity that the RMP deems appropriate. The RMP, at the beginning of the consultation, must inform the patient about his name and qualifications as well as display his registration number prominently accorded to him by the State Medical Council/MCI, on prescriptions, website, electronic communication (WhatsApp/email, etc.) and receipts, etc. given to the patients. Moreover, the RMP must put in place a mechanism that allows the patient to verify its credentials.
Are teleconsultations only allowed between patient and RMP?
No. The Guidelines allow for teleconsultations between the following:
Patient and doctor via a caregiver: In cases where the patient is a minor or is incapacitated (such as in dementia or physical disability) the RMP will proceed with a consultation to such caregiver. The caregiver needs to have formal authorization or a verified document that establishes his relationship with the patient. A caregiver includes a family member, or any person authorized by the patient to represent him.
Health workers and RMP: A health worker can facilitate a consultation for a patient in a public or private health facility. This takes place only after the health worker has already seen the patient and is satisfied that consultation with the RMP is required. The worker is responsible for collecting the details of the patient, his health problems, examining him and convey the findings to the RMP for his diagnosis. A health worker includes a nurse, Allied Health Professional, Mid-Level Health Practitioner, ANM or any other health worker designated by an appropriate authority.
RMP and RMP: The guidelines encourage consultations between RMPs and specialists for the diagnosis, management, and prevention of diseases of the patient. The RMP seeking consultation shall be responsible for the treatment and other recommendations given to the patient. The types of consultations include:
(i) Tele-radiology: sending x-rays, PET scans, MRI scans, ultrasound reports from one location to another.
(ii) Tele-pathology: sending pathology data between distant locations for diagnosis, education, and research.
(iii) Tele-ophthalmology: gives access to eye specialists for patients in remote areas, including ophthalmic disease screening, diagnosis, and monitoring.
No. The Guidelines allow for teleconsultations between the following:
Patient and doctor via a caregiver: In cases where the patient is a minor or is incapacitated (such as in dementia or physical disability) the RMP will proceed with a consultation to such caregiver. The caregiver needs to have formal authorization or a verified document that establishes his relationship with the patient. A caregiver includes a family member, or any person authorized by the patient to represent him.
Health workers and RMP: A health worker can facilitate a consultation for a patient in a public or private health facility. This takes place only after the health worker has already seen the patient and is satisfied that consultation with the RMP is required. The worker is responsible for collecting the details of the patient, his health problems, examining him and convey the findings to the RMP for his diagnosis. A health worker includes a nurse, Allied Health Professional, Mid-Level Health Practitioner, ANM or any other health worker designated by an appropriate authority.
RMP and RMP: The guidelines encourage consultations between RMPs and specialists for the diagnosis, management, and prevention of diseases of the patient. The RMP seeking consultation shall be responsible for the treatment and other recommendations given to the patient. The types of consultations include:
(i) Tele-radiology: sending x-rays, PET scans, MRI scans, ultrasound reports from one location to another.
(ii) Tele-pathology: sending pathology data between distant locations for diagnosis, education, and research.
(iii) Tele-ophthalmology: gives access to eye specialists for patients in remote areas, including ophthalmic disease screening, diagnosis, and monitoring.

How much information has to be shared by the patient?
The type and extent of the information that has to be shared by the patient depends on the RMP’s professional discretion. RMP can request the patient to provide medical history, reports, records, etc. to exercise proper clinical judgment. For e.g. the RMP may ask a diabetic patient to provide him with his blood reports, blood sugar tests, etc. This information can be sent by the patient either through conversation with a healthcare worker/provider or via technology-based tools. However, if the RMP feels that the information received is inadequate, then he can request for additional information from the patient. He may recommend the patient to go for further tests and submit the reports when received. In such instances, the telemedicine is resumed after the required information is received.
What are the duties of the RMPs? What is the penalty if they fail to perform these duties?
The RMPs must uphold and practice the principles of medical ethics, professional norms for protecting patient privacy and confidentiality as per the Indian Medical Council Act as are applicable in physical consultations. They must fully abide by the Ethics Regulations, provisions of the Information Technology Act, 2000 including Information Technology (Reasonable security practices and procedures and sensitive personal data or information) Rules, 2011 and any other applicable rules and regulations. Further, the RMPs are required to maintain the following records/documents:
Phone logs, email records, chat/ text records, video interaction logs, etc.,
Patient records, reports, documents, images, diagnostics, data (digital or non-digital),
In case medicines are prescribed to a patient, then the record of that prescription is to be maintained as required for in-person consultations.
The RMPs can be held guilty of misconduct for all actions that wilfully compromises patient’s care or privacy, or violates any prevailing law including the Guidelines. However, RMPs will not be held responsible for breach of confidentiality if the patient’s privacy have been compromised by a technology breach or by a person other than RMP.
What are the precautions that technology platforms must take note of while providing Telemedicine services?
All the technology platforms (for e.g. mobile apps, websites, etc.) that provide telemedicine services to consumers must ensure that the practitioners on their platform are duly registered with the relevant medical councils. The platforms are required to carry out their due diligence before listing them on their platform. Moreover, the platforms must provide the name, qualification and registration number, contact details of every RMP listed on their platform along with a proper mechanism to address any queries or grievances of the consumers.
Furthermore, artificial intelligence and machine learning based platforms cannot counsel or prescribe any medicine to any patient. Such technologies can only be used to aid and support the RMP, but the final advice and prescription must be made by the RMP.
Any non-compliance may result in the platform being blacklisted by the Board of Governors, MCI.
Is telemedicine expensive?
No, the same fees will be charged for a teleconsultation by the RMP as an in-person consultation.
Can a patient stop/discontinue telemedicine?
Yes, both the patient and the doctor have the right to discontinue telemedicine at any stage.
ABOUT THE AUTHORS
Nikhil Issar is an Associate at PSA, a full-service law firm.
Copyright with PSA and republished with consent for non-commercial purposes
Other Blogs
Online training: Incorporating telemedicine into healthcare practice
Telemedicine refers to providing health care services at a distance using information and communication technologies (ICT). Telemedicine involves providing some kind of health care service to a patient, such as an online consultation between a patient and a doctor, remote patient monitoring through medical devices, or consultations between two doctors to arrive at a management plan for a patient case. The term “telehealth” is a broader umbrella term which encompasses providing health services at a distance (telemedicine) as well as other health system activities like health provider education (eLearning), research and evaluation (online questionnaires), health administration activities. In light of the Covid-19 pandemic, providing health care via telemedicine has become a necessity. The goal of this training is to orient doctors and hospital administrators to the field of telemedicine so they can effectively use telemedicine in their day to day practice or incorporate it into their health organization. This training is open to doctors and health administrators from Asia, Africa and the Middle East.
OBJECTIVES
This training will cover the following topics,
1. Definition of telemedicine
2. Modes which can be used for telemedicine – audio, video, chat, store-and-forward
3. Pros and cons of telemedicine
4. Legal basis of telemedicine
5. Considerations for which drugs can and cannot be prescribed over telemedicine
6. Patient safety and informed consent in telemedicine
7. Advances in telemedicine
8. Demonstration of the Intelehealth platform
9. QnA session
TRAINERS
Dr. Bimal Buch, Chief Medical Officer. M.B.B.S., M.B.A. (H.M.), F.C.G.P., F.P. Consultant, D.H.R.D., P.G.D.H.R.M., P.G.C.H.M.,P.G.C.HIV/AIDS, Dip.T.D. Orange belt Six sigma (MSME), PGC QM & AHO (Post graduate certificate in Quality management and accreditation of Hospital organization), Dip. C.M.H. (NIMHANS)
Watch the recorded training below!

Other Blogs
Proper Hand Hygiene for health workers
Hand hygiene is an important component of infection control. Frequent hand washing is extremely important to protect yourself on the job. The following videos explain the proper techniques for hand washing using soap & water and hand rubbing using sanitizer as per the WHO guidelines.


Don’t have running water at your health facility/home – use this simple innovation called the Tippy Tap!

Hand washing is one of the best ways to prevent the spread of COVID-19. But not everyone has access to running water at all times. The tippy tap is one simple and safe way to wash your hands that is especially designed for areas with no running water. This video produced by WHO Regional office for Africa shows you how!
Other Blogs
Introduction to personal protection measures for health workers
In light of the spread of Covid-19, we are dedicating a series of articles to the use of PPE and other personal protection measures for healthcare workers of all cadres – doctors, nurses, midwives, community health workers, sanitation staff, lab staff to name a few.
This article assumes little to no background in infection control and Personal Protective Equipment (PPE).
HOW INFECTION MAY SPREAD TO A HEALTH WORKER & PRECAUTIONS YOU CAN TAKE
As Covid-19 is an infectious disease which spreads through droplets and fomites, wearing PPE by health care providers is vital for their own protection. When an infected person coughs, droplets spread in the atmosphere, which is why they should wear a mask. But those who are undiagnosed or asymptomatic, they may be spreaders of infection. So health care professionals need to take extra precautions to protect themselves.
Droplets from infected persons may come in direct inhalation during breathing in. So a health worker needs a mask. The average person has 3000 droplets in a single cough that travel at 150 kmph for upto 1-2 meters. Hence, by keeping at least 1-2 meter distance from the patient, you can minimize the risk of getting infected through droplets.
But touching infected surfaces, direct contact with body, belongings and body fluids of patients are real threats to workers. So proper hand washing after each contact with either soap and water or hand sanitizer, as per the situation, is necessary even with all precautions. Even if you have worn gloves, it is recommended that you wash your hands according to hand wash guidelines after removing gloves.

VARIOUS TYPES OF PERSONAL PROTECTIVE EQUIPMENT (PPE)
1. Masks: There are two types of masks available. Triple layer surgical mask and N95 respirator. Both are good for their situations.
1.1. Triple layer mask: The common surgical mask has 3 layers of fabric that is water resistant. This mask can be used for 8 hours. If it gets wet, it has to be removed. Once removed, it has to be disposed of as biomedical waste.
How to use: The mask has a hard metal string on the upper side, which is malleable and is pressed against the nasal bridge to adjust to shape. To cover a large area of face, mouth and nose, it is pleated. On the outer side, these pleats should open downwards, so that there is no pocketing which can lodge droplets near the nose and make the wearer even more vulnerable. Tie the strings behind the head, or there are elastic loops, wear around the ears. Make sure that there is very little space, if any, between mask and face. The mask is not sterile. You can touch any surface when wearing the mask, but once you are ok with it and have started working, you should not touch the front surface of the mask as it is potentially infected. Maneuver the mask with strings. When removing also, touch only the strings.
1.2. N95 respirator mask: This is better in terms of particulate filtration. Fits a bit tightly on the face. May have an expiratory valve and tight texture so that it will not collapse and balloon with respiration.
2. Face shield and goggles: To protect mucous membranes of mouth, nose and eyes from sudden splash of infective material. These also will protect from inadvertent touching eyes, nose and mouth with contaminated fingers.
3. Gloves: When you touch a contaminated surface with bare hands, your hand is likely to be contaminated as well. But this does not replace hand sanitation. Instructions for wearing gloves do not differ. Sterilized gloves are not needed. Usual guidelines for gloves prevail.
Gowns: Body cover is needed to protect the entire body. They are required for workers working in close proximity (less than 1 meter). They have laces to tie from the back. They are akin to surgical gowns used in OT. They are to be used based on risk of exposure.
4. Shoe covers and head covers: As airborne droplets tend to settle, they can catch feet/shoes as well as head.
HOW TO WEAR (DON) AND HOW TO REMOVE (DOFF) PPE PROPERLY
It is extremely important to don and doff PPE properly in order for it to be effective. Hand hygiene is an important aspect of proper PPE removal. Here is a short video explaining the proper sequence as a quick and handy reference. You can also refer to some of the longer videos below.

A short video on the proper sequence of donning and doffing PPE – By Diwakar’s Multispeciality Hospital https://www.divakarshospital.com/ As a healthcare wor…

Authors: Dr. Bimal Buch, Dr. Bhishmaraj Shrivastava and Neha Verma
Other Blogs
Training for NGO staff & volunteers in infection prevention
NGOs that provide essential services like healthcare, food, water, housing, sanitation need adequate infection control measures in place to make sure their staff and volunteers stay safe while also providing their beneficiaries the right information. This online training for health workers/volunteers/field workers offers them adequate knowledge about COVID 19, it’s transmission and preventive measures for public or beneficiaries and themselves. With this knowledge they can perform their activity using adequate protective actions and preventive measures. They can discharge their duties confidently and without fear of acquiring disease from their beneficiaries and also offer protective instructions to beneficiaries.
Interested in organizing a training for your organization?
COURSE CONTENTS
Primary information of virus and disease, mode of spread, clinical features (signs and symptoms), protective measures like social distancing, hand wash, avoid risky touch, cough etiquette, etc. Role of Personal protective equipment, role of isolation and quarantine. Treatment and prophylaxis.
OBJECTIVES
At the end of this discussion, participants will be able to train their staff in activities of Covid-19 epidemic so that they can:
-
Tell signs and symptoms of novel corona virus/COVID 19.
-
Undertake surveillance to identify suspected case of COVID 19.
-
Provide linkage with ASHA/Health workers for further action.
-
Take up proper preventive measures for them selves.
-
Wear triple layer mask as per guidelines.
-
Tell messages of IEC covering all of the points of social distancing, cough etiquette, hand wash and touch care.
-
Demonstrate ability to give messages on role play settings.
After the training is complete, attendees will be sent a post-training quiz. Certificates will be issued to participants on successful completion of the quiz (scoring 80% or higher).
Courtesy: Canva
TIME
1.5 hours
TRAINERS
Dr. Bimal Buch, Chief Medical Officer. M.B.B.S., M.B.A. (H.M.), F.C.G.P., F.P. Consultant, D.H.R.D., P.G.D.H.R.M., P.G.C.H.M.,P.G.C.HIV/AIDS, Dip.T.D. Orange belt Six sigma (MSME), PGC QM & AHO (Post graduate certificate in Quality management and accreditation of Hospital organization), Dip. C.M.H. (NIMHANS)
UPCOMING TRAININGS
Interested in organizing a dedicated training for your non-profit? please fill out our contact form and we will get back in touch with you: https://www.intelehealth.org/contact
Download this poster pack of Covid-19 precautions and put up in your premises, courtesy of Canva
POSTERS
Other Blogs
Intelehealth’s Covid-19 response
Intelehealth is a telemedicine & case management app that supports patients and frontline health workers with a digital assistant called ‘Ayu’ for triage and risk assessment. It connects them with remote doctors over telemedicine (audio/video calls) in order to provide care for patients in hard-to-reach situations. We have set up several telemedicine projects in countries like India, Philippines and Haiti.
We are keeping a close eye on the Covid-19 outbreak in the countries where we work and are actively planning the impact of this outbreak on the programs we support. From the experiences of countries who are battling the pandemic, we believe that the time for preparedness is now, as a late response can be very damaging, especially for vulnerable communities. In our commitment to support strong health systems, we are reaching out to interested health organizations with technical support for Covid response.
Intelehealth’s unique Covid-19 monitoring and case management solution has three modules:
-
Identification of cases:
-
A website for the general public to self-triage and identify if they need to get tested or if they should self-isolate.
-
Available in multiple Indian languages
-
-
Treatment and monitoring of suspected and confirmed cases:
-
A Telemedicine based home-monitoring solution for patients who are suspected or confirmed of having Covid-19 to guide them through the 14 day period of self-isolation/ quarantine. Provides guidance to the patients for how to comply with home-quarantine instructions and health education messages.
-
Features,
-
Allows assigning of health workers to high-risk cases
-
Allows health workers to securely access patient information, update patient medical records with clinical evidence
-
Case Management and medical decisions to recommend isolation can be automated, scaled efficiently using mobile platform
-
-
Mapping of suspected and confirmed cases
-
GIS mapping and real-time monitoring dashboards for suspected and confirmed cases to identify infected clusters
-
Contact tracing module where suspected and confirmed cases can use the app to enter information of the people they have come in close contact with and places they have visited
-

Benefits for Governments, NGOs and hospitals in launching an effective and timely COVID-19 response:
-
Real time data for decision making of level of spread – early warning system to identify community spread
-
Better compliance of patients with home quarantine with less stress
-
Allows greater efficiency in deployment and use of medical resources, doctors attention when appropriate and necessary when meaningful alarms are triggered
-
Availability of credible and strategic data and insights into capacity needs of isolation units
-
Ability to cast a bigger net and have broader reach for COVID-19 response
-
Can inform contact tracing workflows
If you are interested you can contact us via,
Email: covidresponse@intelehealth.io or submit a request via our contact form (select enquiry type as Covid response solution)
=============
Additional links:
-
Track the spread of Covid-19 through this dashboard by the JHU Center for Systems Science and Engineering.
-
For daily situation updates, we like Global Health NOW: https://www.globalhealthnow.org/. Subscribe to their newsletter to get updates in your inbox
-
For how the digital health sector is supporting Covid response check out ICTWorks: https://www.ictworks.org/
Other Blogs
Quality of care & patient safety in telemedicine programs: A toolkit

“First, do no harm”. Patient safety and quality is a cornerstone of healthcare service delivery, yet every 5 minutes patients die because of unsafe care. It is important to safeguard the quality and safety of care delivery in all healthcare environments. To err is human, and it is but natural to assume that to “telemedically” err is human too. On the occasion of the first ever World Patient Safety Day we present a quality index for provider-to-provider telemedicine programs.
Telemedicine can connect patients directly with remote doctors (patient to provider telemedicine) or can connect frontline health providers with doctors or specialists (provider to provider telemedicine) when distance and/or time separate the two. It has demonstrated an improvement in access to healthcare at lower costs. The WHO Digital Health Guidelines recommend the use of provider to provider telemedicine as an evidence-based intervention for health systems strengthening in low and middle income countries.
However despite the rapid growt
How we developed this toolkith of telemedicine, there is not much data on patient safety and the quality of care delivered in this setting. Many studies have raised questions about the comparison of quality of telemedicine as compared to in-person visits. Quality assessment and continuous improvement are important in an in-person clinical setting, and have resulted in major gains in patient safety, improvement in patient satisfaction and health outcomes. There are several quality measures that have been developed for in-person clinical settings, but not many in a telemedicine context.
Intelehealth is a digital health and telemedicine platform supporting frontline health workers. We believe in the cause that ‘everyone should be able to access the health services they need, when and where they need them, without facing any financial hardship’. By developing an app & open source telemedicine software, we ensure that the frontline health workers are able to significantly reduce the time, distance, money, and effort spent by patients to access health care. To evaluate the quality of healthcare offered and to understand it’s sustainability, we have come up with an extensive Clinical Quality Metrics for monitoring and evaluating the quality of healthcare at our projects. A major goal in developing this Clinical Quality Index for Telemedicine was to achieve quality improvement, improve health outcomes and reduce preventable harm for people utilizing the telemedicine service, keeping in mind their safety and wellbeing.
These metrics help a telemedicine program to:
-
Provide an objective standard for measuring the program quality and achieve continuous quality improvement
-
Measure and record the efficacy and effectiveness of the system or process
-
Establish & monitor best practices for patient safety to reduce preventable harm
Other Blogs
Five Families. Five Stories. Five Ways We Can Improve the Healthcare System.
Globally, the public healthcare systems have monitored and planned several targeted (vertical) interventions for specific diseases like tuberculosis, malaria, anemia and for certain disadvantaged groups like women and children through primary healthcare programs. These vertical programs have resulted in a number of big wins, one such example being a global reduction in maternal and child mortality. However, health systems have become more complex over time with a number of such selective programs for many health areas – like maternal health, child health, non-communicable diseases, communicable diseases. Often there is very little connection between these health programs and each operate in its own way. Several groups of people are also frequently neglected like those with disabilities, needing mental healthcare and the aging (geriatric) population.
We at Intelehealth, do our bit by using/developing technology to deliver comprehensive primary health care to underserved communities in remote and far-flung areas. We work to integrate technology and comprehensive primary healthcare supported by digital health tools. Last week, a part of our team visited Umerga and a few other villages in Osmanabad (Maharashtra, India). It was a routine baseline survey but in the end, what we experienced in these rural areas, deeply moved each one of us. Here are five of the most touching stories from the field that, in a way, shaped our thinking of what introducing comprehensive primary health care here would mean to them.
1. Comprehensive care means addressing the underlying social issues that lead to poor health
“Can you tell me what’s wrong with her?” pleaded an upset middle-aged woman as she pulled her daughter closer to come and sit with us. “Take a look at her. She can’t even walk properly and she gets irritated so easily. We couldn’t even send her to school, let alone make her stay there. She has been like this since she was born”. The hapless young girl, who looked to be around 16 years old, seemed to have some kind of developmental disability. However, the family simply wasn’t aware of what to do and where to go and get help for her. They had sought advice from their relatives, some doctors, and even faith healers. But in the end, they did not know what to do, condemning the girl to a life of isolation.
The problem solved- Social issues like lack of awareness of stigmas prevalent about mental illnesses is a major barrier to seeking care. Health promotion and awareness is a part of CPHC that would have positively impacted the life of such people with disabilities
2. Comprehensive care means focusing on early diagnosis and prevention and not just cure
“My wife has a lump in her breast from the past 3 years. But I think the treatment will be too expensive and tedious. From where do I get the money? And who would look after my wife in the hospital? So we haven’t gone to see any doctor,” said a poor farmer as his wife curiously peeked in from the kitchen.
Just a few houses away, a young woman, we interviewed, shared how she recently attended a screening camp for cervical cancer and menstrual abnormalities. She was screened positive for a possible lump in her uterus and was referred to a hospital for further investigation. “My family didn’t want me to go. They said there was no need as I was perfectly fine. But I didn’t listen to them and went anyway.” Further tests showed she did not have cancer and the lump was benign. But she was proud that she stood up for herself.
The problem solved- Women usually face a lot of social and cultural barriers and because of which they don’t speak up for their health. Screening programs, part of CPHC, can help promote positive health-seeking behavior in disadvantaged communities.
3. Comprehensive care is sensitive to the needs of all age groups, including neglected groups like the elderly
An 80-year old lady sat down next to us, and not realizing we weren’t doctors, began to pour out her heart on her ailment, i.e. how she was having a lot of difficulties during swallowing. “I even went to a big hospital in Pune. But the doctor said he would have to put a big tube down my throat and check! I got so scared I never went back. Now I am finding it so hard to swallow.”

The problem solved- Lack of education and awareness often hold people back from seeking the treatment they need, and especially in the elderly. Additionally, it becomes very difficult for them to travel far and they are dependent on other family members for tending to their needs. Also, being uneducated, having deep-seated cultural biases and the dearth of public health programs for the geriatric population, makes matters worse. Health education and promotion helps such people to understand their ailments and how to help themselves out.
4. Comprehensive care includes lowering out-of-pocket expenses for patients
“I had kidney stones, and we spent close to Rs. 18000 for my treatment, but I still have a lot of discomfort and still sometimes in pain. I may have to go back but I am worried about the toll it would have.” The farmer we were talking to, ran inside his house and came back with a new insurance card under the Pradhan Mantri Jan Arogya Yojana (Ayushman Bharat scheme). “I made this new card. But I do not understand it. What do I do with this? Can I use this for my treatment? I went to a hospital but they said they don’t accept this card. Can you help me understand this?”
The problem solved- Often financing schemes do not reach beneficiaries or they may not know how to access them or in this case, how to use it. A health system that focuses on comprehensive care also looks into how care can be made affordable. However, education regarding insurance have still not percolated through the rural masses and could be a training point.
5. Community health workers (CHWs) can be a powerful medium to deliver comprehensive care

“I saw this young pregnant woman who was very weak. While she had been at her mother’s home, she was being well taken care of. She would regularly come to the Primary Health Center for her checkups during pregnancy,” said a midwife (a type of CHW in India). “But after she came to her mother-in-law’s home, she was prevented from coming for her regular checkups. I went to her house and told her mother-in-law that she needed to care for her daughter-in-law like her own daughter. I told her I would bring the village elders to her home and make sure she was held responsible if anything happened to her daughter-in-law.” We realised that CHWs can be a powerful force to address underlying social issues like these.
The problem solved- Health seeking behaviour i.e. preventive medicine is usually not a part of the treatment process and the patients usually approach the doctor after exhausting all home remedies and out of fear. The CHWs can effectively promote positive health-seeking behavior through screening, raising health awareness and home visits. CHWs bring the health system to the doorstep of patient, and are an agent for change in the way the community perceives healthcare.
Other Blogs